Visceral Fat, Inflammation, and the Metabolic Risk Most People Are Missing
Metabolic Health Series | Issue 04
There's a number that most of us have been conditioned to focus on: the one on the scale. It gets checked at the doctor's office, it anchors our sense of whether we're doing well or doing poorly, and it drives more dietary decisions than almost any other metric.
Here's the problem: body weight is a poor predictor of metabolic health. You can be thin and metabolically compromised. You can carry extra weight and be metabolically robust. What matters far more than how much fat you carry is where you carry it — and what that fat is doing. In my 1:1 work with clients I urge everyone to have a body composition Dexa scan that tells us exactly how much lean mass, fat mass and visceral fat they carry.
This issue is about visceral fat: what it is, why it's so metabolically significant, how to assess your actual risk, and what moves the needle on reducing it.
Not All Fat Is the Same
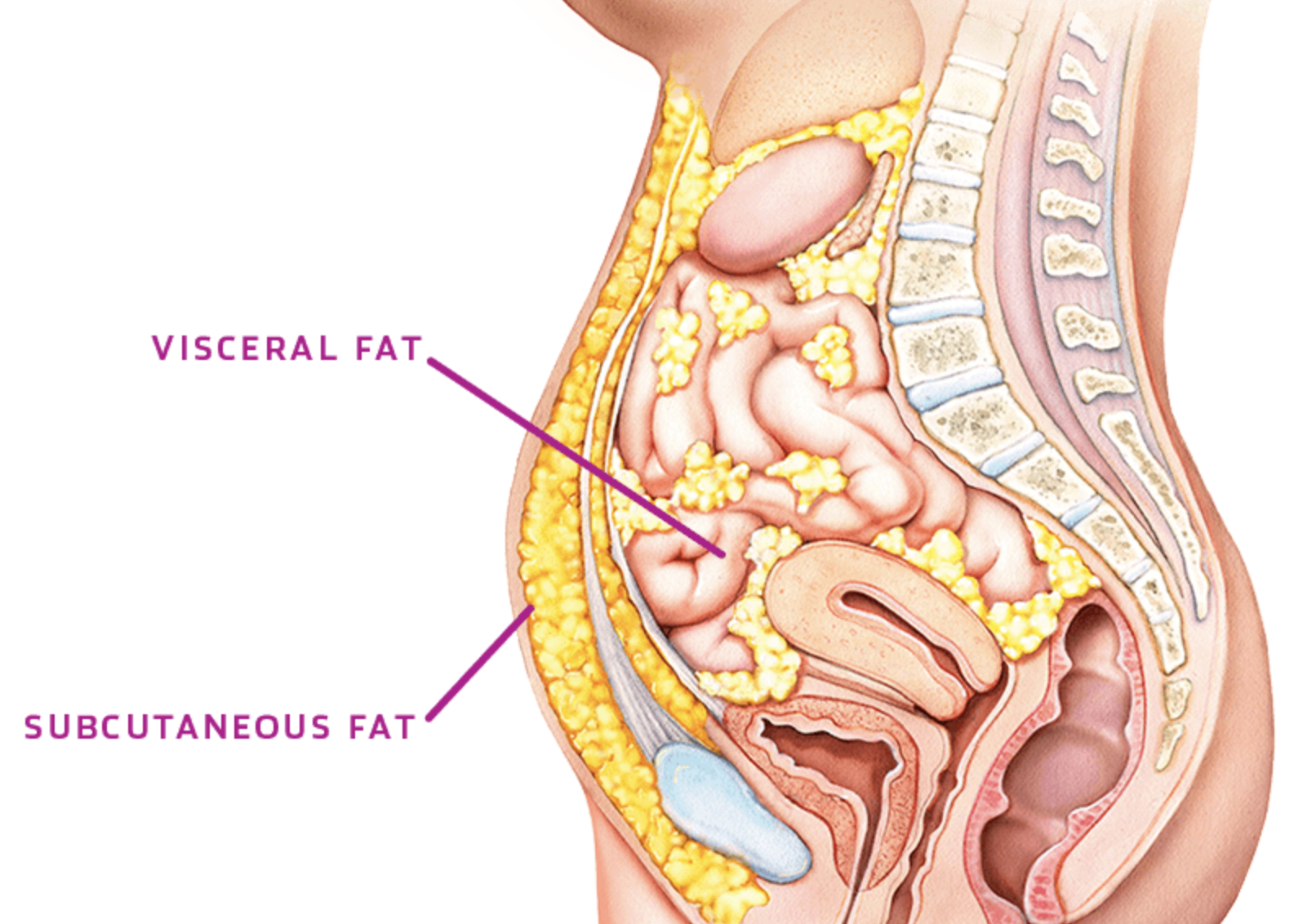
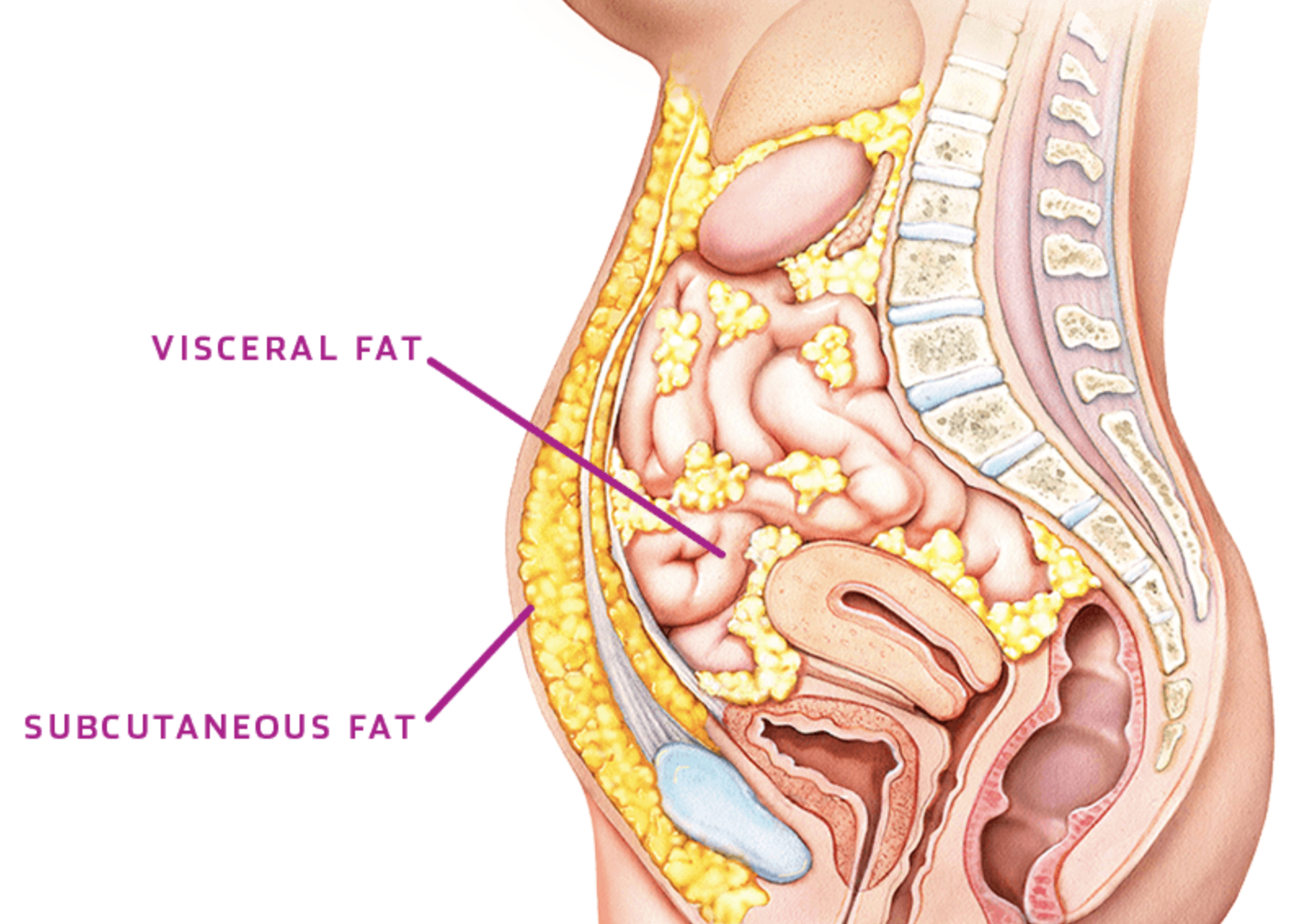
Body fat exists in distinct compartments, and they behave very differently.
Subcutaneous fat sits just beneath the skin — on the hips, thighs, arms, and buttocks. It's the fat you can pinch. While excess subcutaneous fat has its own metabolic implications, it is relatively inert compared to its deeper counterpart and may even offer some protective functions in certain contexts.
Visceral fat sits deep inside the abdominal cavity, packed around the liver, pancreas, intestines, and other vital organs. You cannot see it or pinch it. Someone can look relatively lean and carry significant amounts of visceral fat — a pattern sometimes called TOFI (thin outside, fat inside) — which is precisely why relying on appearance or body weight alone is so misleading.
The distinction matters because visceral fat and subcutaneous fat are functionally different tissues. Visceral fat is not passive storage. It is a metabolically active endocrine organ — and an inflammatory one.
Visceral Fat as an Endocrine Organ
This framing — fat as an endocrine organ — is one of the most important conceptual shifts in metabolic science over the past two decades. Visceral fat doesn't just sit there. It actively secretes hormones and signaling molecules called adipokines, which circulate through the body and influence metabolism, immunity, and organ function.
When visceral fat accumulates and becomes dysfunctional, its adipokine output shifts in a damaging direction:
Leptin — the satiety hormone — is produced in excess, leading to leptin resistance, in which the brain stops responding to the "I'm full" signal despite high levels circulating in the blood
Adiponectin — an anti-inflammatory, insulin-sensitizing hormone — is suppressed; lower adiponectin is one of the most reliable markers of metabolic risk
TNF-α and IL-6 — pro-inflammatory cytokines — are released in elevated quantities, contributing to systemic chronic inflammation
This inflammatory output is what creates the bridge between excess visceral fat and the downstream diseases associated with metabolic syndrome: cardiovascular disease, type 2 diabetes, non-alcoholic fatty liver disease, and certain cancers. The fat isn't simply a storage problem — it's an active signaling problem.
Biomedical researcher Dr. Rhonda Patrick has extensively documented how this kind of chronic low-grade inflammation impairs mitochondrial function — the powerhouse in our cells responsible for energy production. When mitochondria are compromised by inflammatory signaling, cells become less efficient at burning fuel, less responsive to insulin, and more prone to the kind of metabolic dysfunction that increases over time. It's a downstream consequence of visceral fat that most people never connect to the tissue in their abdomen.
A Better Way to Assess Risk
The most useful tool for assessing visceral fat risk isn't expensive or complicated — it's a tape measure.
Waist-to-height ratio has strong research support as a predictor of cardiometabolic risk across diverse populations and body types. A 2012 systematic review involving more than 300,000 adults found it significantly outperforms waist circumference alone for predicting diabetes, hypertension, and cardiovascular disease in both men and women. The reason is intuitive: it captures central fat distribution — where the metabolic risk actually lives — and scales naturally across different body sizes.
The threshold is simple to remember: keep your waist circumference to less than half your height. A ratio above 0.5 warrants attention; above 0.6 represents significantly elevated risk.
What Drives Visceral Fat Accumulation
Visceral fat doesn't accumulate randomly. It responds to specific metabolic inputs — the same ones that drive metabolic syndrome more broadly:
Chronically elevated insulin. As covered in Issue 2 of this 12-part series, hyperinsulinemia directly promotes fat storage, and visceral fat depots are particularly insulin-responsive. Diets high in refined carbohydrates and added sugars are among the strongest dietary drivers of visceral fat accumulation.
Elevated cortisol. Visceral fat cells contain a higher density of cortisol receptors than fat cells elsewhere in the body. Chronic stress — and the sustained cortisol elevation that accompanies it — preferentially drives fat into abdominal storage. This is the physiological mechanism behind the phenomenon many people experience: significant life stress followed by noticeable abdominal weight gain (cortisol belly), independent of dietary changes.
Poor sleep. Even modest sleep deprivation raises cortisol, disrupts appetite hormones, and promotes visceral fat accumulation. The relationship between sleep quality and visceral fat is dose-dependent — the less and worse you sleep, the more visceral fat tends to accumulate over time.
Physical inactivity. Skeletal muscle actively competes with visceral fat for metabolic resources. When muscle mass is low or sedentary, visceral fat has less metabolic competition — and more room to expand.
Alcohol. Alcohol is processed almost entirely by the liver, and regular consumption — even at moderate levels — promotes liver fat accumulation and visceral adiposity through pathways similar to those Lustig described for fructose in Issue 2.
Measuring What Actually Matters
Beyond waist-to-height ratio, there are several other practical ways to track visceral fat and metabolic risk without expensive imaging:
Waist circumference alone — measured at the navel, not the narrowest part of the torso — remains a useful standalone marker. Above 35 inches for women and 40 inches for men is considered elevated risk by standard guidelines, though these cutoffs may underestimate risk in certain ethnic groups.
Triglyceride-to-HDL ratio — available from a standard lipid panel — is one of the most sensitive blood-based proxies for visceral fat and insulin resistance. A ratio above 2.0 suggests insulin resistance is likely present; above 3.0 is significantly elevated. This single calculation often tells more of the metabolic story than many more complex tests.
Fasting insulin — as discussed in Issue 1 — reflects the degree to which the pancreas is compensating for insulin resistance, which closely tracks with visceral fat burden.
For those who want precision, a DEXA scan (dual-energy X-ray absorptiometry) can quantify visceral fat directly and measure lean muscle mass alongside body fat — providing a complete body composition picture that no scale can match.
What Actually Reduces Visceral Fat
The research here is consistent and encouraging: visceral fat is more metabolically responsive to intervention than subcutaneous fat. It tends to be lost first and fastest with the right inputs.
Reduce refined carbohydrates and added sugars. Lowering dietary carbohydrate load reduces insulin, which directly reduces the primary hormonal driver of visceral fat storage. This is the most targeted nutritional intervention for visceral adiposity.
Prioritize resistance training. Building and maintaining skeletal muscle increases the body's insulin-independent glucose disposal capacity and creates metabolic competition with visceral fat stores. Multiple studies show that resistance training reduces visceral fat even in the absence of significant weight loss.
HIIT — specifically the Norwegian 4x4 protocol. Rhonda Patrick has been emphatic on this point: when it comes to dropping visceral fat in the shortest amount of time, high-intensity interval training outperforms steady-state cardio. The Norwegian 4x4 — developed by researchers at the Norwegian University of Science and Technology — involves four intervals of four minutes at 85–95% of maximum heart rate, each followed by three minutes of active recovery at 60–70% of max heart rate. The full session takes roughly 25 minutes including warm-up and cool-down. Beyond visceral fat reduction, consistent use of this protocol has been shown to boost VO2 max by up to 13% over eight weeks and can reduce the biological age of the heart by up to two decades. Two to three sessions per week is the target.
Here she is talking about losing visceral fat:
https://www.youtube.com/watch?v=ShxhtskaHck&t=2s
Improve sleep quality. Extending sleep duration and improving sleep quality — we’ll tackle this in depth in Issue 7 — reduces cortisol, normalizes appetite hormones, and directly reduces visceral fat accumulation over time.
Manage cortisol. Given the density of cortisol receptors in visceral fat, chronic stress management is a direct anti-visceral-fat intervention, not an indirect one. The somatic and nervous system practices discussed in Issue 3 are as relevant here as they are for hormonal health.
Three Things to Do This Week
Measure your waist-to-height ratio today. Measure your waist at the navel (relaxed, not sucked in), divide by your height in the same units. If it's above 0.5, you have useful information. If it's above 0.6, that warrants a conversation with your healthcare provider.
Pull your last lipid panel and calculate your triglyceride-to-HDL ratio. Divide your triglycerides by your HDL. Above 2.0 is a signal worth acting on.
Try a modified Norwegian 4x4 session this week. Pick any cardio modality — walking briskly uphill, cycling, swimming, or even stair climbing. Alternate four minutes of hard effort (breathing heavy, can barely speak) with three minutes of easy recovery. Repeat four times. That's it — 25 minutes, and you've done one of the most evidence-backed things available for visceral fat reduction.
Next issue: "Eat Like Your Metabolism Matters" — an evidence-based nutrition framework for reversing metabolic syndrome, including the dietary patterns with the strongest research behind them and a simple structure for building metabolic meals.
This newsletter is educational and does not constitute medical advice.
Have you had a body composition DEXA scan?

Lisa Marlene Thompson is a Functional Nutritional Therapy Practitioner, somatic facilitator, and health and lifestyle guide for anyone ready to feel more alive in their body. With advanced certifications in menopause science with Dr. Stacy Sims, somatic movement with Michaela Boehm, and sleep and brain health informed by the research of Lisa Mosconi and Matt Walker, her work sits at the intersection of cutting-edge science and deep body wisdom.
Her signature program — Strength, Sleep & Sensuality — is an invitation to come home to your body: to build real strength, reclaim restorative sleep, and rediscover a nervous system that is grounded and provides aliveness in the body that belongs to this chapter of life. She is based in Los Angeles and works with clients worldwide.
Your most vibrant chapter is still ahead.
I'd love to explore what's possible together → Reach out: lisa@lisamarlenethompson.com